
Understanding Nasal Problems
Many people struggle with nasal congestion and stuffiness, making it difficult to breathe properly. Chronic congestion often leads to mouth breathing, especially at night, which can result in a dry mouth and disrupted sleep. Several issues can cause nasal congestion, such as allergies or narrow nasal passages. One common cause of narrow passages involves the nasal septum and turbinates.
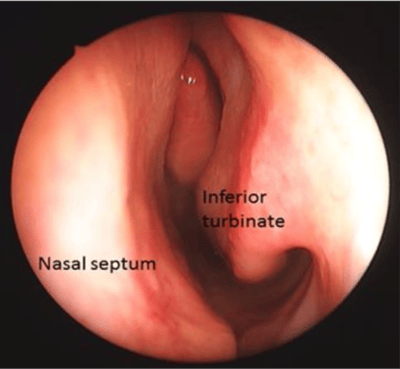
The nasal septum is a structure dividing the nasal passages into right and left sides. Turbinates are structures inside the nose, close to the septum, helping regulate airflow. However, if turbinates are too large, they can obstruct airflow, leading to nasal congestion.
Deviated Nasal Septum
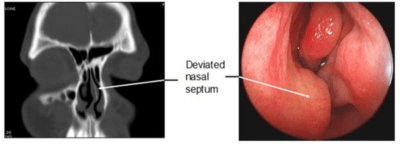
The septum is made of cartilage and bone, covered by a thin membrane called mucosa, similar to skin inside the nose. When the septum bends or curves, it’s called a deviated nasal septum. This deviation can block one or both sides of the nose, causing significant symptoms. Surgery, known as septoplasty, can help correct this deviation and improve airflow. However, surgery isn’t necessary for everyone with a deviated septum; it’s recommended when symptoms are severe.
Diagnosis
A doctor can diagnose a deviated septum through a thorough evaluation, including a nasal endoscopy, which examines the nasal passages. Sometimes, a CT scan may be necessary. Treatment options, including surgery, can be discussed once diagnosed.
Surgery
During septoplasty, the surgeon straightens the cartilage and bone, often removing portions if needed. This procedure aims to improve nasal airflow, typically performed under general anesthesia in an outpatient setting. Recovery involves managing mild pain and stuffiness, with some patients requiring packing inside the nose during healing.
Inferior Turbinate Hypertrophy
Turbinates are structures on the side wall of the nose, helping warm and moisturize air. Enlarged inferior turbinates can block airflow, leading to nasal congestion. Diagnosis involves a nasal endoscopy, with treatment options including medication or surgery if symptoms persist.

Surgery
Turbinate reduction surgery aims to shrink the turbinates. Various methods exist, such as cauterization or submucosal resection, often performed alongside septoplasty. Surgery can be done in-office or in the operating room. Post-operative care involves managing mild discomfort and stuffiness, with potential for temporary numbness or pain in the teeth or tip of the nose.
Risks of Septal and Turbinate Surgery
As with any surgery, there are risks, including bleeding, persistent symptoms, infection, tooth and nose numbness, septal perforation, brain fluid leak, or rare changes in smell, taste, or voice.
Combining Septoplasty with Turbinate Reduction
In many cases, endoscopic sinus surgery is combined with septoplasty and turbinate reduction to improve overall nasal airflow. Septoplasty corrects a deviated septum, while turbinate reduction reduces the size of swollen turbinates that block airflow. Combining these procedures with sinus surgery can enhance symptom relief, improve breathing, and reduce the risk of post operative congestion. Patients often experience faster and more complete recovery, as multiple underlying nasal issues are addressed in a single procedure. This approach is particularly beneficial for individuals with chronic nasal obstruction, recurrent sinus infections, or structural abnormalities contributing to their sinus disease.
Insurance Coverage and Candidacy
Endoscopic sinus surgery is typically covered by most health insurance plans when medically necessary. Candidacy is determined based on persistent symptoms, failed medical therapy, and imaging evidence of sinus blockage or chronic disease. Insurance approval often requires documentation of chronic sinusitis, nasal polyps, or structural obstruction, along with failed treatments such as medications, nasal sprays, or irrigations. Your ENT specialist can guide you through the pre authorization process, helping ensure coverage and clarifying any out of pocket costs. Proper documentation and evaluation also ensure that patients receive surgery only when it is medically indicated and likely to provide meaningful symptom relief.
Common Questions
How can I find out what is causing my nose blockage?
Nasal endoscopy helps diagnose nasal blockage causes. Treatment options vary, depending on the cause. An ENT specialist can determine if surgery is necessary.
Will my nose be broken during a septoplasty?
In septoplasty and turbinate surgery, procedures focus on the inside of the nose, without breaking the nose or causing external bruising.
Copyright © 2020 by the American Rhinologic Society