
Epistaxis
Epistaxis is when you bleed from your nose. The nose has a lot of blood vessels because it needs to warm and moisten the air we breathe before it reaches the lungs. When a blood vessel bursts, it causes bleeding. Nose bleeds are very common, with more than 60% of people having had nosebleeds at some point. Epistaxis is divided into two types based on where the bleeding is coming from. Nosebleeds can come from the front (Anterior) or back (Posterior) of the nose. Most nosebleeds (90%) come from the front of the septum, the wall that divides your nose, and is easy to control. A small number of nosebleeds (5-10%) come from the back of the nose and are more challenging to fix. Most nosebleeds are not serious and stop on their own.
Why do nose bleeds happen?
Several things can cause nosebleeds. The most common cause is irritation or damage to the lining inside of the nose. This can be caused by dry air, trauma, or misusing nasal sprays. Minor trauma to the nose, such as from picking or blowing the nose too hard, and more significant events, such as nasal surgery, can cause bleeding. Several factors can increase the risk of getting a nosebleed, including taking blood thinners like aspirin or warfarin, high blood pressure, and dry climate. In some cases, nosebleeds can be a symptom of an underlying medical condition, such as blood clotting disorders (hemophilia or hereditary hemorrhagic telangiectasia) or nasal tumors.
How are nose bleeds diagnosed?
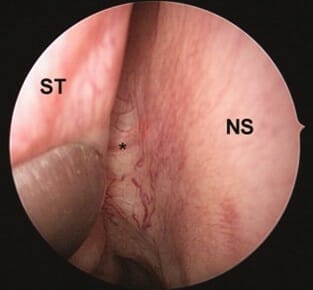
To determine how serious your nosebleed is and whether you need treatment, the doctor will ask questions about your medical history and the nosebleeds. They may look into your nose using a special light and/or camera (called nasal endoscopy) to see where the bleeding is coming from.

How are nose bleeds stopped?
If you have an active nosebleed, lean forward and pinch the lower, soft part of the nose for at least 5 minutes and up to 15-20 minutes. This is usually effective for stopping most nose bleeds. Applying pressure on the hard, bony portion of the nose will not be effective. Leaning the head back will cause the blood to get into the lungs, so this should be avoided. Over-the-counter nasal decongestant sprays like oxymetazoline (pronounced ok-see-muh-taz-uh-leen) or phenylephrine (pronounced fen-l-ef-reen) can slow down nosebleeds. However, these sprays must not be used for more than a few days.
If these methods don’t work, your doctor may use sticks coated with a chemical called silver nitrate to cauterize (or burn) the blood vessels shut. They may also use electrical cautery in some instances. Another way to control nose bleeds is packing the nose. Packing can be made of a material that dissolves or does not dissolve, which must be removed later. If the nosebleed is more complicated, your doctor may recommend a procedure called embolization to block off a blood vessel using a special material. Another option is surgery, which may involve endoscopically tying off or cauterizing a bigger blood vessel in the nose.

How can nose bleeds be prevented?
Applying sprays, ointments, and gels to the front of the nose daily helps to moisturize the nose. This prevents nosebleeds due to dryness. It is important to avoid any trauma after a nosebleed. Picking scabs or blowing the nose too aggressively can cause another bleed.
When Should I See a Doctor about a Nosebleed?
If you have a heavy or long-lasting nosebleed that keeps coming back, or if you feel weak or dizzy and the bleeding stops you from doing your normal activities, you should see a doctor.
Importance of Nasal Endoscopy Evaluation
A nasal endoscopy evaluation allows your ENT specialist to closely examine the nasal passages and sinus openings using a thin, flexible camera. This procedure helps accurately diagnose sinus blockages, polyps, or inflammation, guiding effective treatment plans and ensuring that interventions like medications or surgery are precisely targeted for optimal results.
Summary
There are different ways to treat nosebleeds. Non-surgical treatments, such as applying pressure and decongestants, usually work well. If these do not help, doctors may use other methods like packing or burning the blood vessels. If the nosebleed is very severe or does not stop with other measures, the doctor may recommend special procedures such as embolization or surgery. For more information on epistaxis, visit the American Academy of Otolaryngology’s Epistaxis guidelines for patients and ENTHealth.
Links:
https://aao-hnsfjournals.onlinelibrary.wiley.com/doi/10.1177/0194599819889945
https://sinushealth.com/conditions/sinus-tumors/
https://sinushealth.com/treatments/nasal-endoscopy/
https://www.enthealth.org/conditions/nosebleeds/