
What is fungus?
Fungi are plant-like creatures all around us, in the soil, our homes, and the air we breathe. Some fungi are good for us and keep us healthy. Most people with healthy immune systems are not affected by fungi. However, in rare cases, the fungus may cause inflammation in the nose and the sinuses (called fungal rhinosinusitis), similar to symptoms caused by mold in the sinus cavity. Fungal allergies can also cause other allergic diseases like allergic fungal rhinosinusitis, which can have different symptoms and need different treatments.
What Is Allergic Fungal Sinusitis?
Allergic fungal sinusitis is a form of chronic rhinosinusitis driven by an allergic immune response. The body reacts to inhaled fungal spores by producing thick allergic mucin inside the sinus cavities. Over time, this buildup blocks drainage pathways and leads to pressure, congestion, and nasal polyps.
This condition is different from:
-
Fungal ball, where fungal material collects in a single sinus cavity.
-
Invasive fungal sinusitis, which is rare and occurs mostly in people with weakened immune systems.
In allergic fungal sinusitis, the fungus does not invade or destroy tissue. The inflammation is caused by the immune system itself.
How Allergic Fungal Sinusitis Develops
Allergic fungal sinusitis develops when the immune system overreacts to naturally occurring fungal spores in the environment. These microscopic spores are inhaled daily and normally do not cause problems. However, in susceptible individuals, the immune system identifies these fungi as harmful and triggers an exaggerated inflammatory response.
This immune reaction leads to the production of thick allergic mucin inside the sinus cavities. Allergic mucin is a dense, sticky material made up of inflammatory cells, mucus, and fungal debris. As this material accumulates, it blocks the normal drainage pathways of the sinuses. When drainage is obstructed, air cannot circulate properly, and pressure begins to build.
Different types of fungal sinus infections:
Overall, fungal sinusitis can be classified into two categories: invasive and non-invasive. Non-invasive fungal sinusitis only stays in the sinuses and does not spread to other areas, while invasive fungal sinusitis can potentially spread to neighboring parts. Invasive fungal sinusitis is very rare.
Noninvasive versions include:
- Fungal ball, where fungus or mold collects in one or more of the sinus cavities. The fungus ball can eventually get big enough to block the sinuses.
- Allergic fungal rhinosinusitis is when you have an allergy to fungus or mold. There can be a lot of mucus buildup and sinus polyps can form.


Invasive versions are very rare, but more serious. They include:
- Acute Invasive Fungal Sinusitis, where the fungus or mold spreads through the blood vessels into the sinus tissues and bones, roof of mouth, eye, and brain. Fortunately, it is extremely rare. It progresses quickly and can cause symptoms such as numbness in the face, double vision, blindness, and changes in awareness levels if it reaches the brain. It tends to strike people whose immune systems do not function well, such as people with poorly controlled diabetes with high blood sugars, people who are undergoing chemotherapy, organ transplant recipients, and people with immunodeficiencies.
- Chronic Invasive Fungal Sinusitis, where the fungus or mold invades the sinus tissue and bone but progresses slowly. It doesn’t cause many side effects or death, and it is usually found in people with normal immune systems.
- Granulomatous Invasive Fungal Sinusitis is similar to CIFS but with specific changes in tissues and the types of people it affects. It’s typically found in people with typical immune systems in North Africa, the Middle East, and Asia and can cause the eye to protrude or be displaced.

Allergic Fungal Sinusitis Symptoms to Watch For
Allergic fungal sinusitis commonly presents with the following symptoms:
- Pressure or pain in the face
- Headache
- Nasal congestion or obstruction
- Discolored nasal drainage
- Foul-tasting postnasal drip
- Reduced sense of smell or taste (with allergic fungal rhinosinusitis)
Acute invasive fungal sinusitis symptoms are described separately above. In some cases, patients may experience noticeable facial swelling if sinus blockage becomes severe. Symptoms often recur even after multiple courses of antibiotics, which is a key sign that the condition is allergy driven rather than bacterial.
How Allergic Fungal Sinusitis Is Diagnosed
Diagnosing allergic fungal sinusitis requires a combination of clinical evaluation, imaging studies, and laboratory findings. ENT specialists rely on well-established diagnostic criteria to confirm the condition.
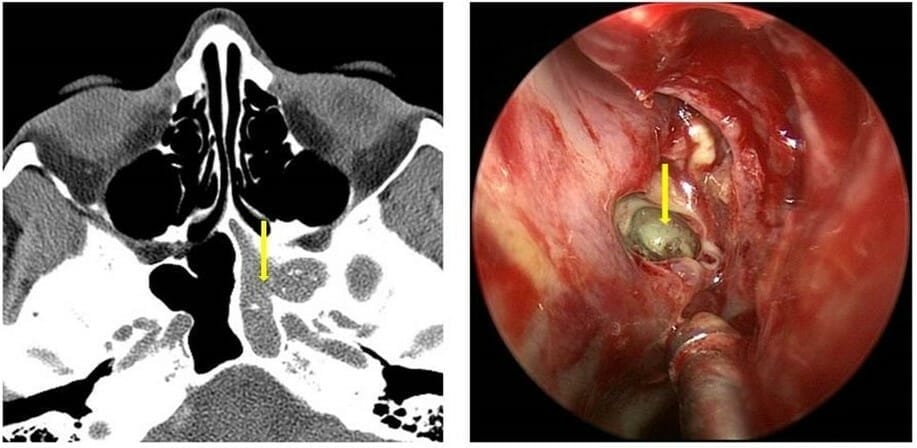
A CT scan of the sinuses often shows areas of dense material within the sinus cavities. This material represents allergic mucin and fungal debris. Sinuses may appear expanded due to pressure from long-standing inflammation. Nasal polyps are commonly present.
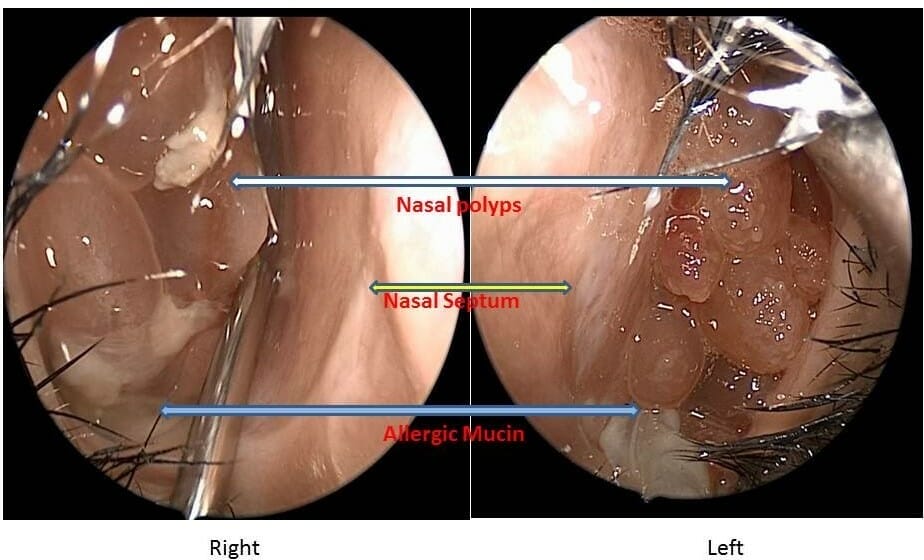
During nasal endoscopy, thick allergic mucin may be seen within the sinus passages. This mucin often has a peanut butter–like consistency and may contain visible fungal elements under microscopic examination.
Blood tests may show elevated IgE levels, reflecting an allergic response. Allergy testing frequently confirms sensitivity to environmental molds. Unlike invasive fungal sinusitis, there is no tissue invasion or bone destruction caused by the fungus itself.
Proper diagnosis is important because allergic fungal sinusitis requires both surgical and long-term medical management to prevent recurrence.
Allergic Fungal Sinusitis Treatment Options
In allergic fungal sinusitis, surgery is often necessary to remove the fungus. The extent and urgency of surgery depend on the type of infection. Endoscopic sinus surgery is usually effective for allergic fungal sinusitis and other non-invasive types of fungal sinus disease. You can learn more about the signs to watch for in our guide on 7 telltale symptoms of allergic fungal sinusitis. Emergency endoscopic or open surgery is required for acute invasive fungal sinusitis, as it progresses rapidly and can be fatal.
After surgery, it is important to irrigate the sinuses regularly to keep them clean. The doctor may also prescribe steroids to reduce inflammation and antibiotics to treat co-existing bacterial infections. Antifungals are necessary for treating invasive fungal sinusitis and are not typically recommended in all other types of fungal sinusitis. Allergy shots may be recommended for allergic fungal rhinosinusitis.
Long Term Management and Recurrence Risk
Allergic fungal sinusitis is a chronic condition with a tendency to recur if not carefully managed. Even after successful endoscopic sinus surgery, ongoing inflammation can return without appropriate medical therapy.
Long-term management typically includes daily saline irrigations and consistent use of topical corticosteroid sprays or steroid rinses. These treatments help reduce inflammation and prevent the reaccumulation of allergic mucin.
Regular follow-up visits with nasal endoscopy allow specialists to monitor healing and remove early buildup before significant blockage occurs. In patients with severe or recurrent disease, biologic medications that target specific inflammatory pathways may be considered.
It is important to understand that antifungal medications are not routinely used for allergic fungal sinusitis. Because the condition is driven by an allergic immune response rather than an active tissue infection, controlling inflammation is the primary goal.
With proper surgical care, allergy management, and long-term follow-up, most patients experience significant symptom improvement and reduced recurrence rates.
The bottom line
Most sinus infections are caused by viruses or bacteria. However, in some individuals, fungi can trigger a chronic allergic inflammatory response known as allergic fungal sinusitis.
Allergic fungal sinusitis is a chronic allergic condition that often requires surgery and long-term anti-inflammatory management. Early diagnosis improves outcomes and reduces recurrence.
With proper diagnosis and consistent care, patients can achieve significant symptom relief and long term sinus control.
Links:
https://sinushealth.com/conditions/nasal-polyps/
https://sinushealth.com/conditions/adult-sinusitis/
https://sinushealth.com/treatments/nasal-endoscopy/
https://sinushealth.com/treatments/sinonasal-irrigations/
https://sinushealth.com/find-a-rhinologist/
https://sinushealth.com/conditions/anosmia-smell-and-taste-disorders/
https://sinushealth.com/treatments/endoscopic-sinus-surgery-2/
https://sinushealth.com/resources/anatomy/sinus-anatomy/